REFERRING PATIENT FORM
Fields with an * are mandatory.
This field is mandatory!
This field is mandatory!
This field is mandatory!
This field is mandatory!
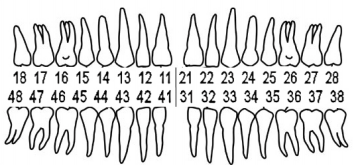
Upper Right Quadrant
Upper Left Quadrant
Lower Right Quadrant
Lower Left Quadrant
This tooth/teeth require(s) root canal therapy:
This Tooth/Teeth Require(s) Retreatment:
Existing Crown/Bridge
Crown will be Replaced
This field is mandatory!
Please fill in all fields with an asterisk.
Form was sent successfully. Soon we will get in contact with you.


